
Nourish and the Decade of Consumer Health
A Case Study in How to Build a $1B+ Consumer Health Business

Weekly writing about how technology and people intersect. By day, I’m building Daybreak to partner with early-stage founders. By night, I’m writing Digital Native about market trends and startup opportunities.
If you haven’t subscribed, join 70,000+ weekly readers by subscribing here:
Nourish and the Decade of Consumer Health
A few years ago I had the chance to interview Priscilla Chan for a fireside chat. Priscilla Chan is best known as Mark Zuckerberg’s wife; beyond her marriage, she tends to keep a low profile. But Chan has a unique career herself: she’s a pediatrician (who still actively practiced medicine until just a few years ago) and co-CEO of the massive Chan-Zuckerberg Institute (CZI), which has a $220B endowment. This means she’s operated at both extremes of scale.
Given those unique vantage points—both seeing patients 1-on-1 in a hospital and spending $1B+ a year through CZI—I wanted to ask Chan a question about depth of impact vs. breadth of impact.
I framed the question with a story about my brother, Carson. Carson is a urogyn, a surgical subspecialty in obstetrics / gynecology. Our mom passed away from ovarian cancer when I was one and Carson was three, so it’s a little poetic that he ended up working in women’s health: one procedure that urogyns do is remove the fallopian tubes to reduce the risk of ovarian cancer. (I’m a proud brother!)
Anyway: Carson is a terrific human and as you’d expect, he cares a lot about depth of impact. He loves the tangible nature of his job, how he can feel his direct impact on a patient. Working day in and day out in a hospital, you’re operating at the atomic level of impact for the healthcare system. That’s what energizes Carson: the depth and tangibility of his work.

I, meanwhile, have been steeped in the Kool Aid of tech and business, which are all about breadth of impact—disrupt, innovate, fix the broken system, and so on. I get energized thinking in terms of years vs. the day-to-day. My question for Priscilla: How do you toggle between depth and breadth? Do your two very different roles (doctor and philanthropist) reinforce each another or create tension?
Her answer has stuck with me. “To have effective breadth of impact,” she said, “you have to first intimately understand depth of impact.” She gave an example:
Working in San Francisco General Hospital, Chan noticed that one variable most influenced whether her patients would receive care. Was the BART running on time? (BART, which stands for Bay Area Rapid Transit, is the local public transit system.) If the BART was delayed, Chan’s patients wouldn’t risk missing work and they’d skip their doctor’s appointment. Only by working at the atomic level did Chan learn which variable was most critical, which then informed large philanthropic investments into public transit.

I like this story because it helps me wrap my head around both sides of healthcare: how care is actually delivered, at the molecular level, and the broader systems that dictate care. Brace yourself for the tech analogy in 3, 2, 1…
The internet is, in many ways, like the BART. When people in Silicon Valley are trying to sound fancy, they call the internet “the rails.” As in, “We need new rails for healthcare delivery in America.” The metaphor here is obvious. The internet reinvents how we can deliver care (and as a bonus, the internet doesn’t break down or operate with delays).
Yet healthcare has been slow to adopt technology because of red tape and bureaucracy. COVID was an important change agent (more on that later) and now we have AI coinciding with telehealth as reinforcing technologies. The time is ripe for very large healthtech companies to be built.
In this week’s Digital Native I want to give a case study of how technology is changing healthcare in real time. We’ll talk about Nourish, a Daybreak company and one of the fastest-growing healthcare companies in the world.
Case Study: How Nourish Nailed the Healthcare Triad
I tend to think about healthcare as a triangle.
There are more cooks in the kitchen than this, and this is clearly an oversimplification, but healthcare really breaks down to three core players: patients, providers, and payers.
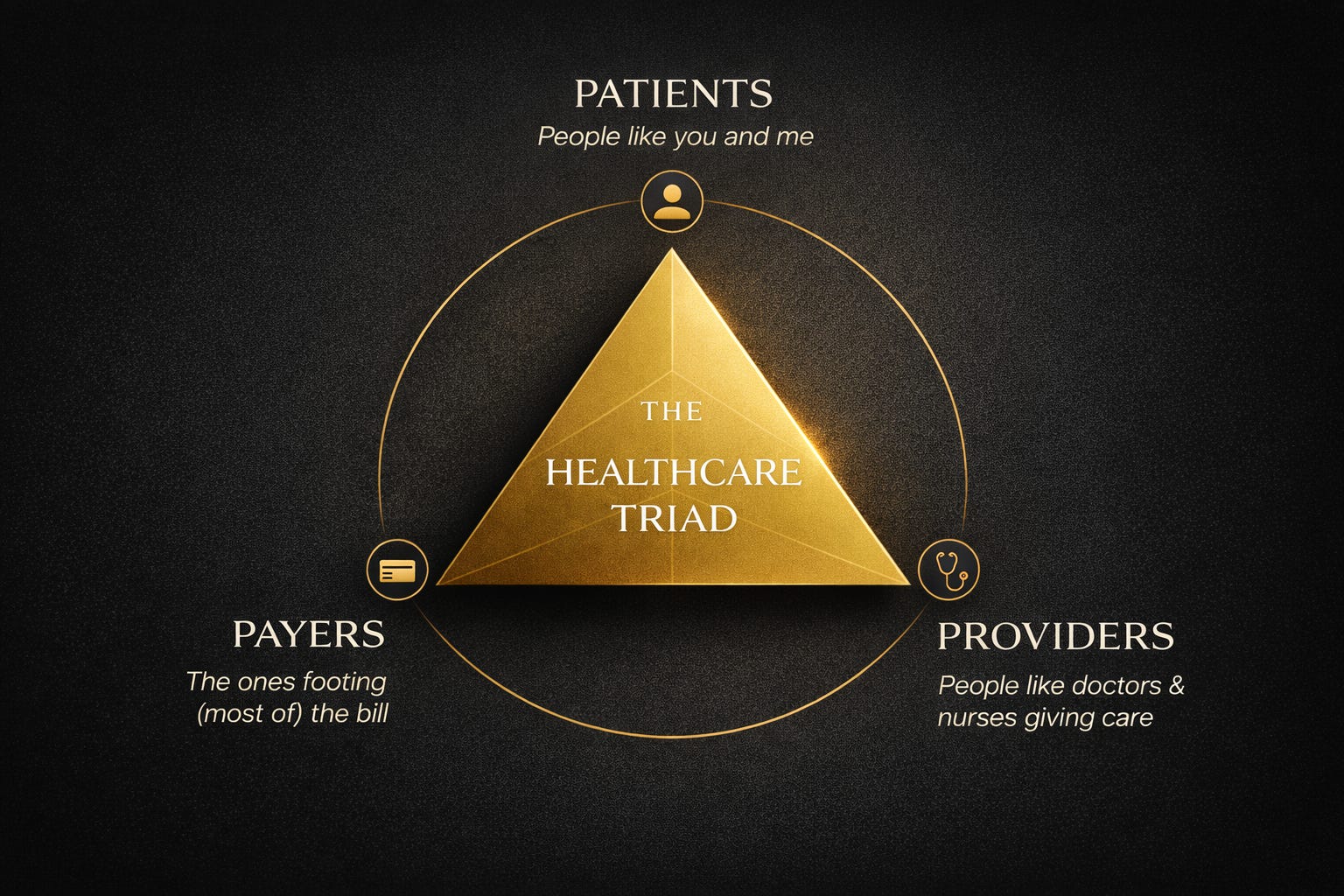
Patients get care. Providers deliver care. And payers pay for a big chunk of that care.
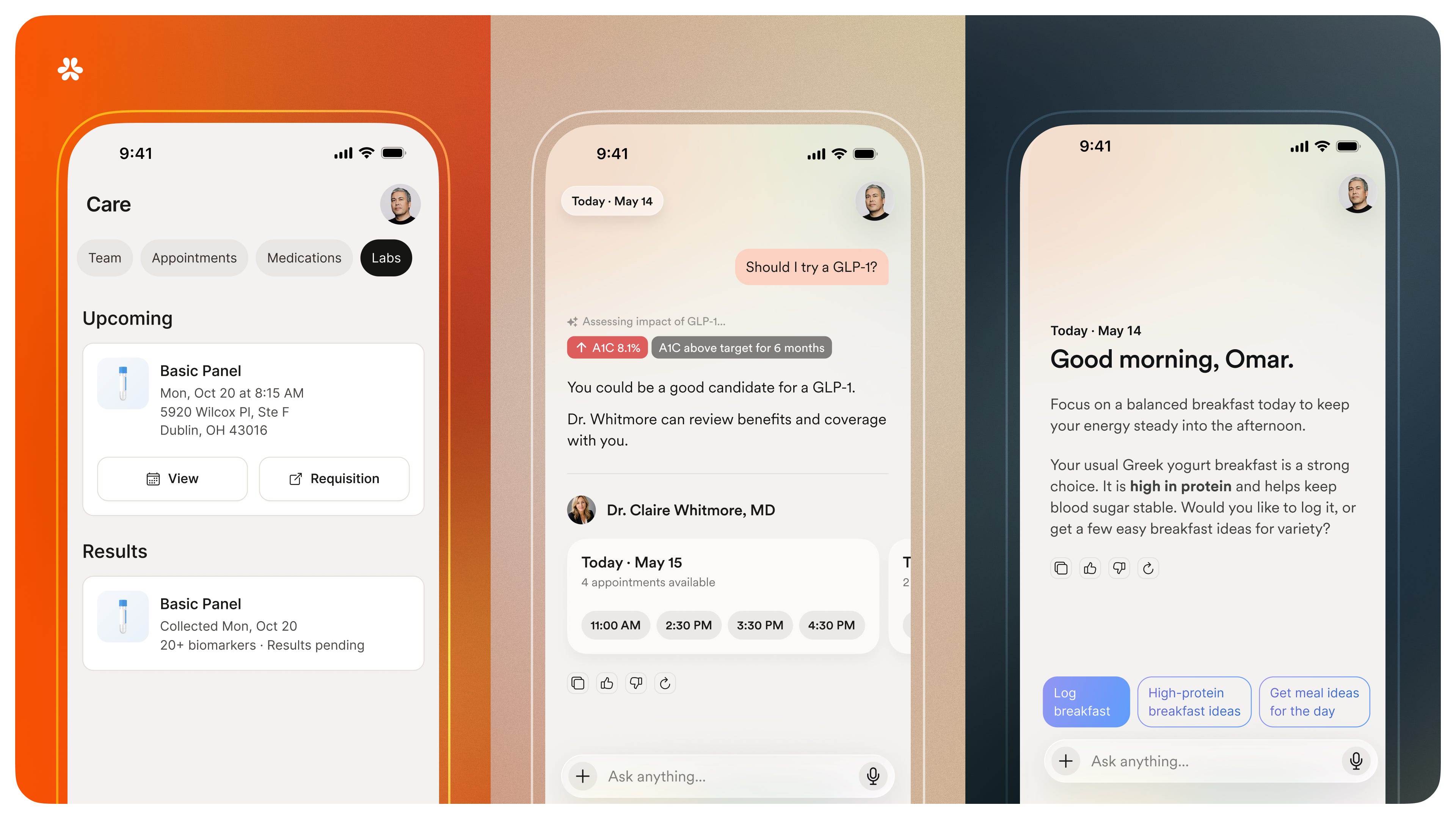
At its simplest, Nourish is a company that lets you talk to a dietitian and get it covered by your insurance. It’s the category leader in telenutrition.
But this description is misleadingly narrow. I would reframe it: Nourish began by connecting you with a dietitian, but is becoming a healthcare juggernaut that nails all three sides of the triangle. The company: (1) has built a beautiful and intuitive consumer-facing product; (2) created a platform that underpins work for over 10,000 of providers; and (3) struck massive, national payer partnerships that broaden access to affordable healthcare with >200M covered lives.
Nourish’s co-founders—Aidan Dewar (CEO), Sam Perkins (President), and Stephanie Liu (CTO)—have executed relentlessly to build what I think is one of the most underrated startups operating today. The goal of this piece to explain how they’ve done it and to draw out some lessons for building in healthcare.

We’ll break this piece into three sections:
The “Why Now” for Nourish
Execution (What Nourish Has Built to Date)
Roadmap (Where Nourish Goes From Here)
The “Why Now” for Nourish
A common theme in Digital Native is the belief that large companies get built when technology shifts intersect with behavior shifts. We’ve written about many examples:
Robinhood rode a technology shift (mobile) that intersected with behavior shifts around people becoming more financially educated, motivated, and independent in a post-Great Recession era.
Instagram also rode the rise of mobile, including rapidly-improving smartphone cameras. At the same time, people were learning to live more public lives, build parasocial relationships, and cultivate global communities / social graphs untethered from geographic constraints.
Figma, meanwhile, rode a technology shift in WebGL (released in 2011, WebGL let you render interactive graphics in the browser) alongside the increasing importance of design in a digital world and the expanding definition of “designer”—online, everyone was becoming a designer.
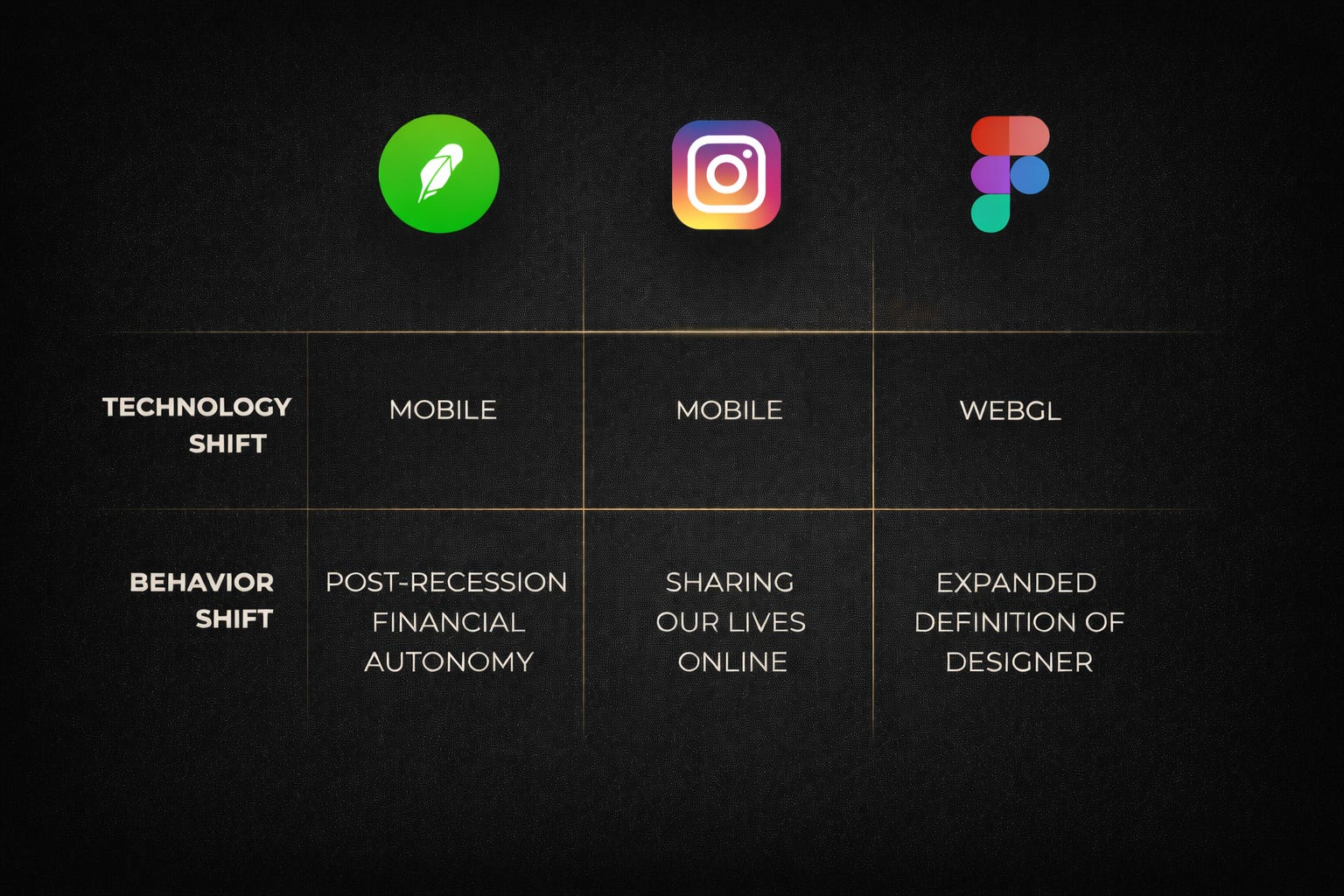
Nourish benefits from three technology shifts (telehealth + AI + medicines) underpinned by arguably the strongest consumer behavior shift of the decade. To take each in turn:
Tech Shift #1: Telehealth
This is the rails analogy. The internet makes it easier to see a provider, and telehealth coverage is expanding rapidly.
COVID was a big catalyst here, with post-COVID telehealth policies making it easier to bill for these codes in virtual visits. The Affordable Care Act was also a factor: as one example, the ACA required coverage for obesity screening and counseling, which pushed more insurers to cover dietitian services. And beyond coverage, adoption accelerated dramatically: 50% of US adults now actively use telehealth.
Tech Shift #2: AI
AI is a more nascent tech shift. On the provider side, AI is already widely adopted by physicians to automate admin work. The patient side is next: while Nourish patients today receive telehealth consultations by human RDs, we aren’t far from a world in which AI consultations can be billed to insurance. You can at least envision a portion of care being handled by AI (for instance, lower-acuity cases or simple questions).
As AI improves, everyone will have an AI doctor, one that knows everything about you and your goals, everything about medicine, one that’s connected to all your health data, and can answer your questions then tell you what to do / share insights proactively / route you to the right care. Today, that level of care is reserved for the wealthy (those with access to concierge doctors, personal trainers, body scans, functional medicine clinics, and private chefs). Startups are making that level of care accessible to everyone.
Tech Shift #3: Medicines
This is the technology shift that’s often overlooked, but that’s as much a function of new breakthroughs as telehealth or AI. GLP-1s are arguably the most successful drugs ever, commercially and culturally. Revenue for Ozempic and Mounjaro has grown even faster than revenue for Anthropic and OpenAI:

We’re in the early innings of adoption: ~2% of eligible patients have access to GLP-1s today.
Behavior Shift: The Consumerization of Healthcare
Forerunner ran a survey that asked consumers to rank life goals in order of priority. Health & Wellness narrowly beat out Friends & Family in importance, which I found (1) a little surprising, and (2) emblematic of the big shift we’re seeing:

People are sick and tired (literally) of healthcare’s status quo, and they’re looking for better options. This is a frequent topic in Digital Native, and our recurring “10 Charts” series has featured many related charts. If we had to sum up America’s healthcare woes in a single chart, it’s probably this one that maps per capita healthcare expenditures against life expectancy:
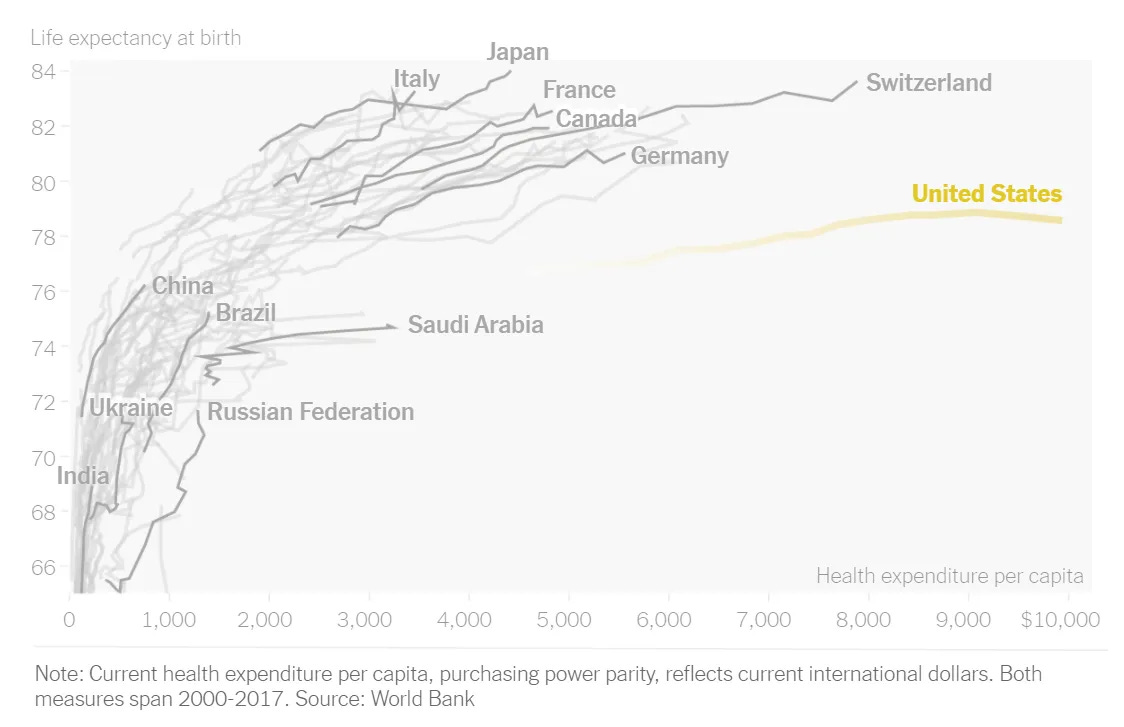
The US… doesn’t look great here. The chart data here is actually a little old: the US now spends about $13,000 (!) per person per year on healthcare, double what countries like the United Kingdom ($5,500) and Canada ($6,300) spend. Yet we’re not getting much bang for our buck.
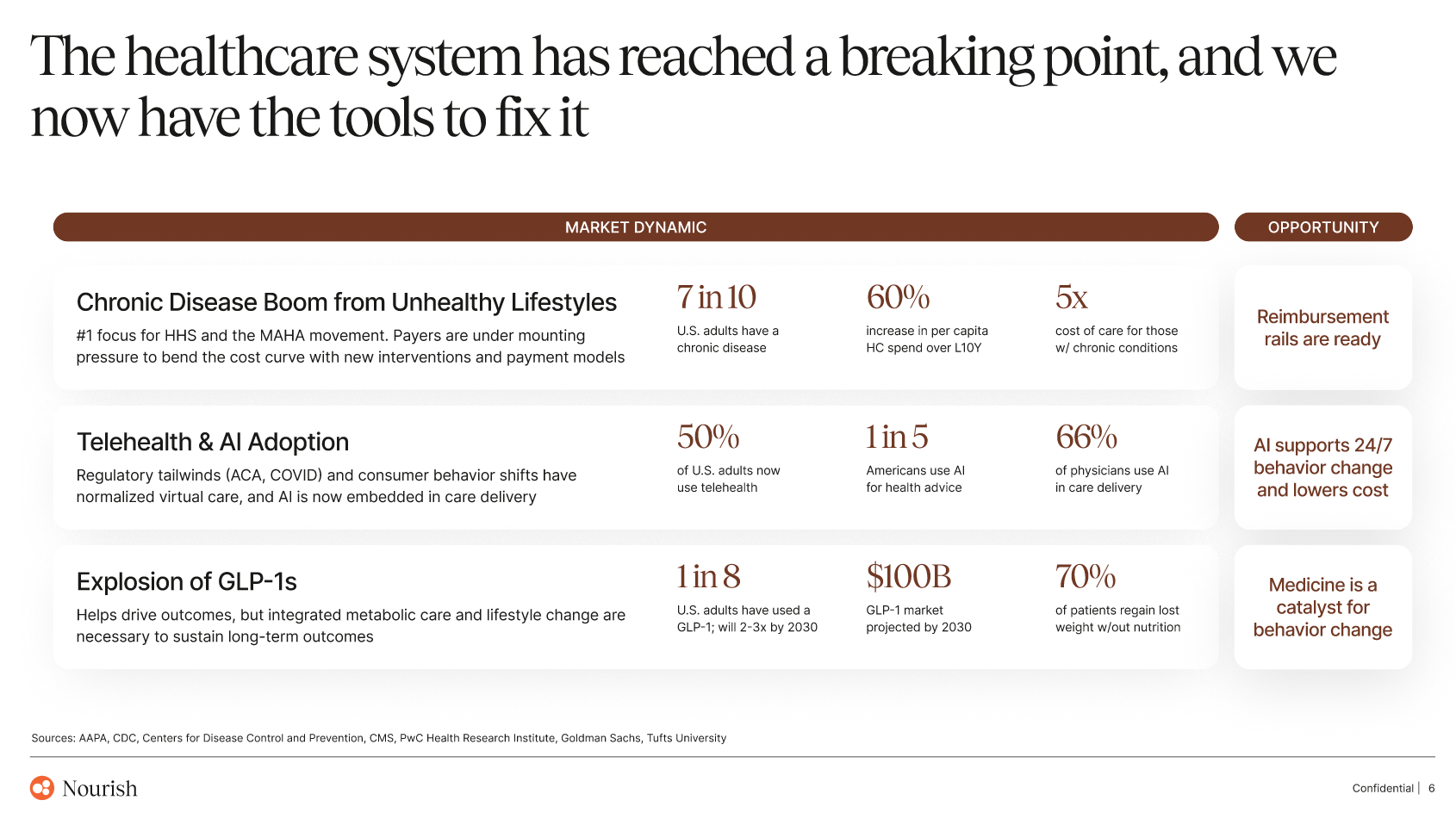
Here’s how Nourish frames it in their deck:
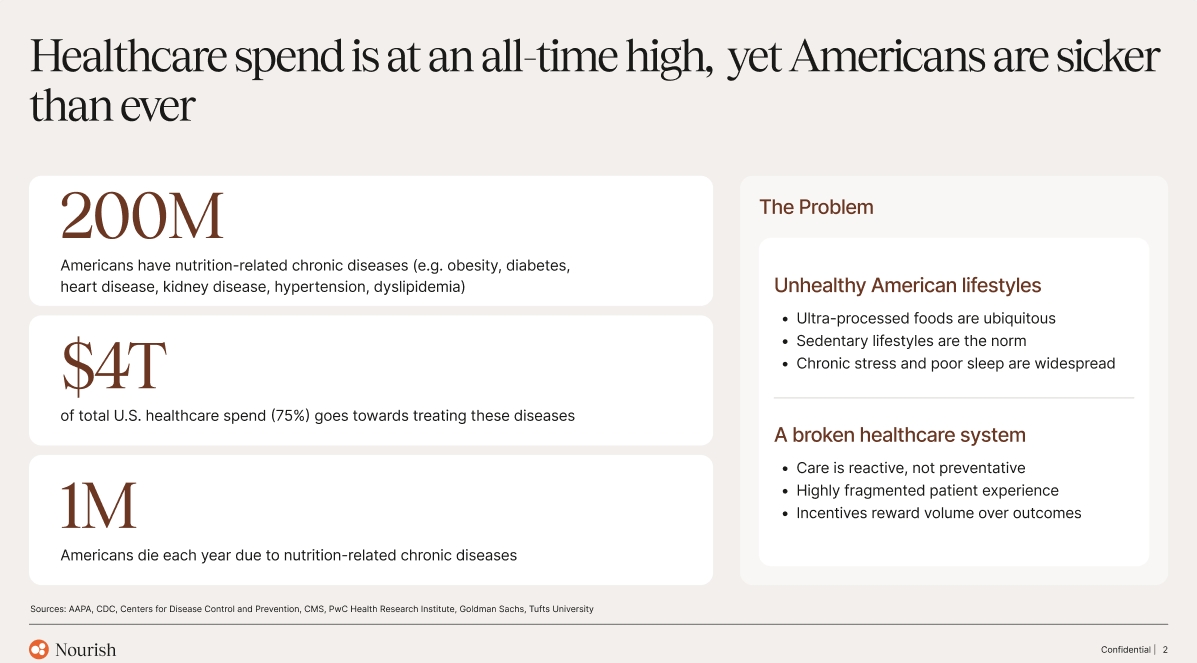
America’s poor health directly ties back to our food supply. Check out this visual:
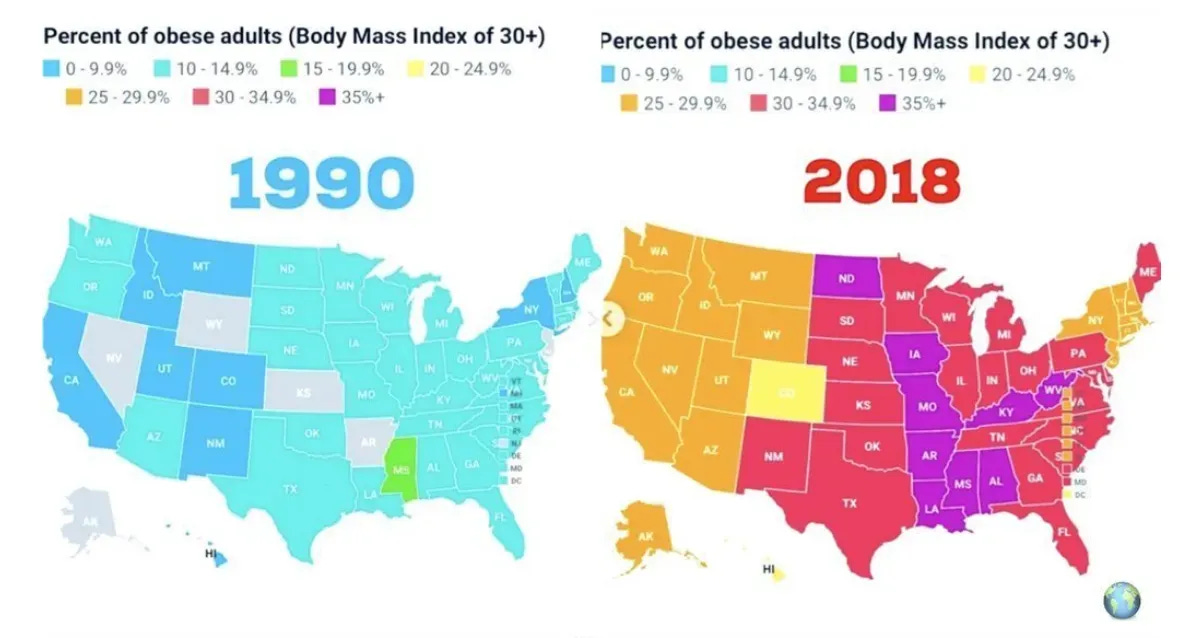
In 1990, zero states had obesity rates above 20%; in 2018, zero states had obesity rates below 20%. (For what it’s worth: 19 states now have obesity rates over 35%.)
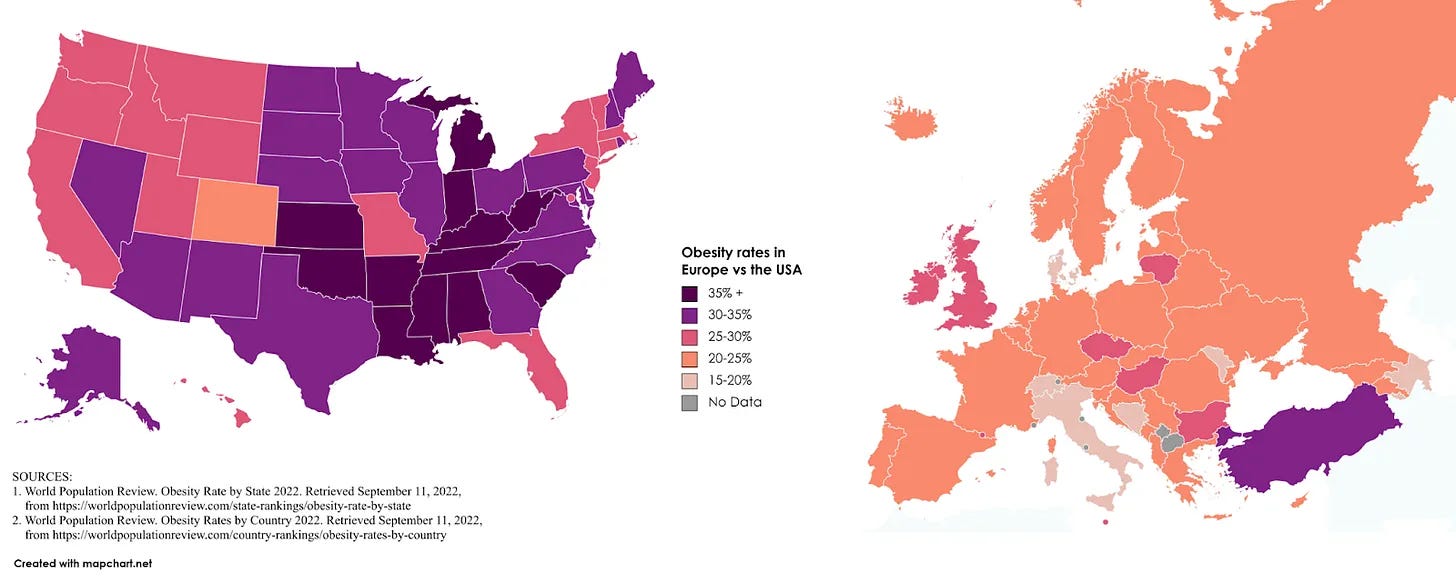
Here’s America compared to Europe:
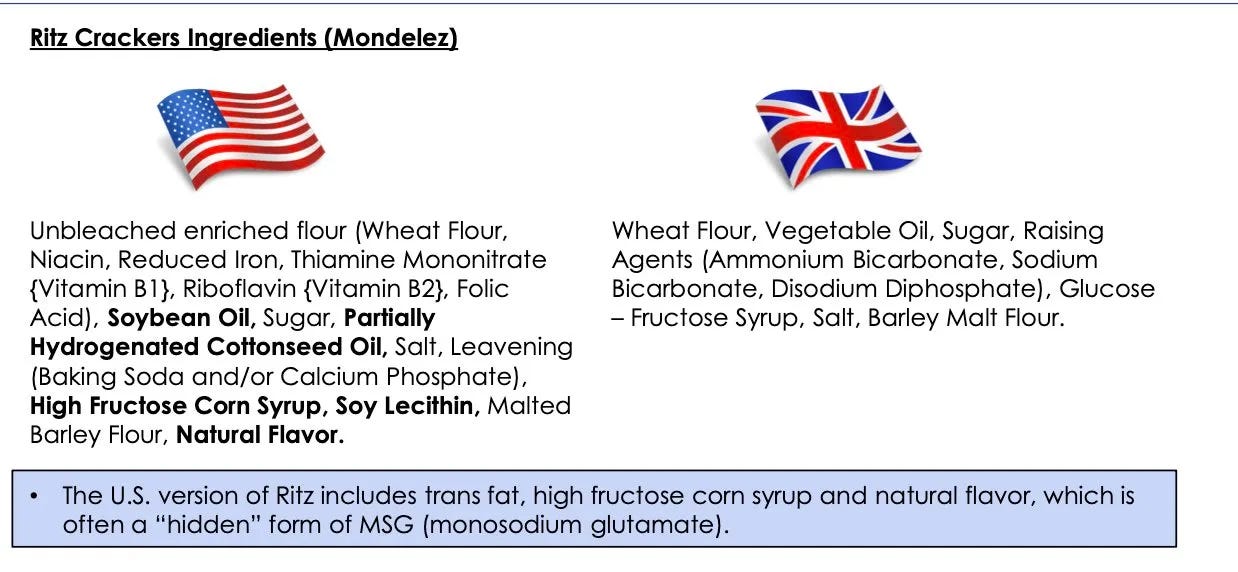
One of my favorite graphics is this one, comparing the ingredients for Ritz Crackers in the US vs. the UK:
We can further see the causality of the food supply on obesity in these charts:
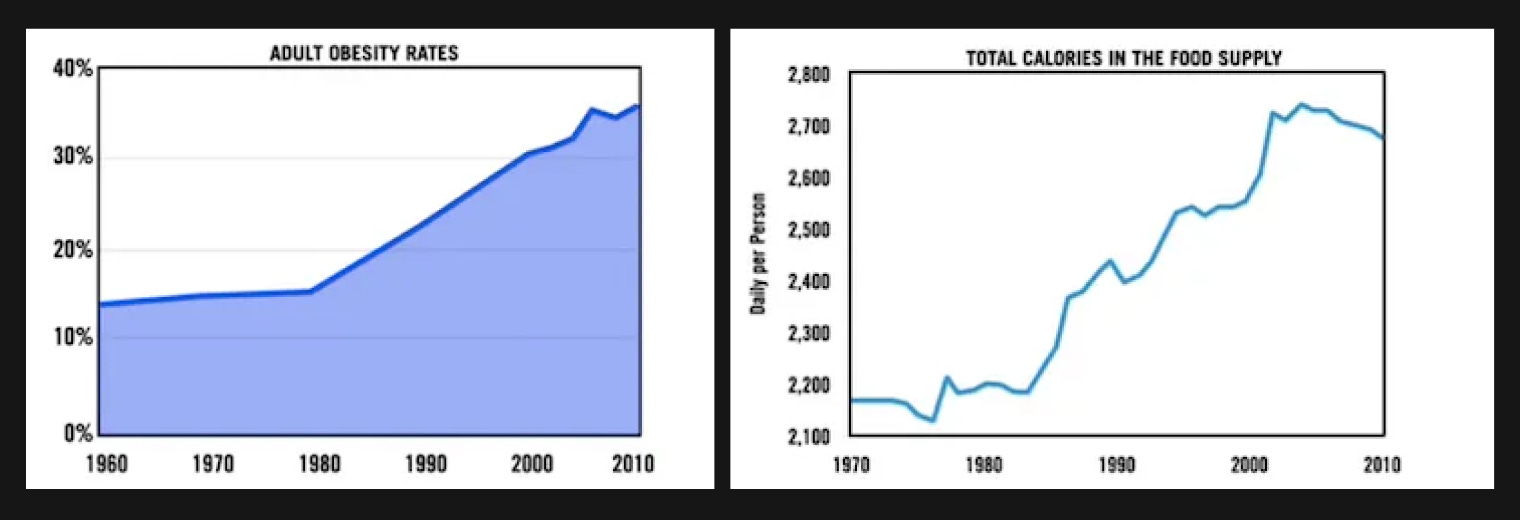
This is only skimming the surface, and Justin Mares has some good writing on this topic. The point is: America is sick, and nutrition is the root cause for chronic disease. So much of healthcare lives downstream of nutrition.
Execution (What Nourish Has Built to Date)
Nourish’s key insight was that nutrition is the root cause of chronic disease, and chronic disease is the root of the aforementioned healthcare problems. Nutrition is the atomic unit here, the depth of impact. Tackle nutrition, and you find yourself at the beachhead of solving systemic problems. From there, you can drive measurable improvements in health outcomes; this is the zoomed out vision, the breadth of impact.
Here’s another chart from the Nourish deck, showing that 7 in 10 US adults have a chronic disease (about 200M Americans) and that those people cost the healthcare system 5x more than the average person:
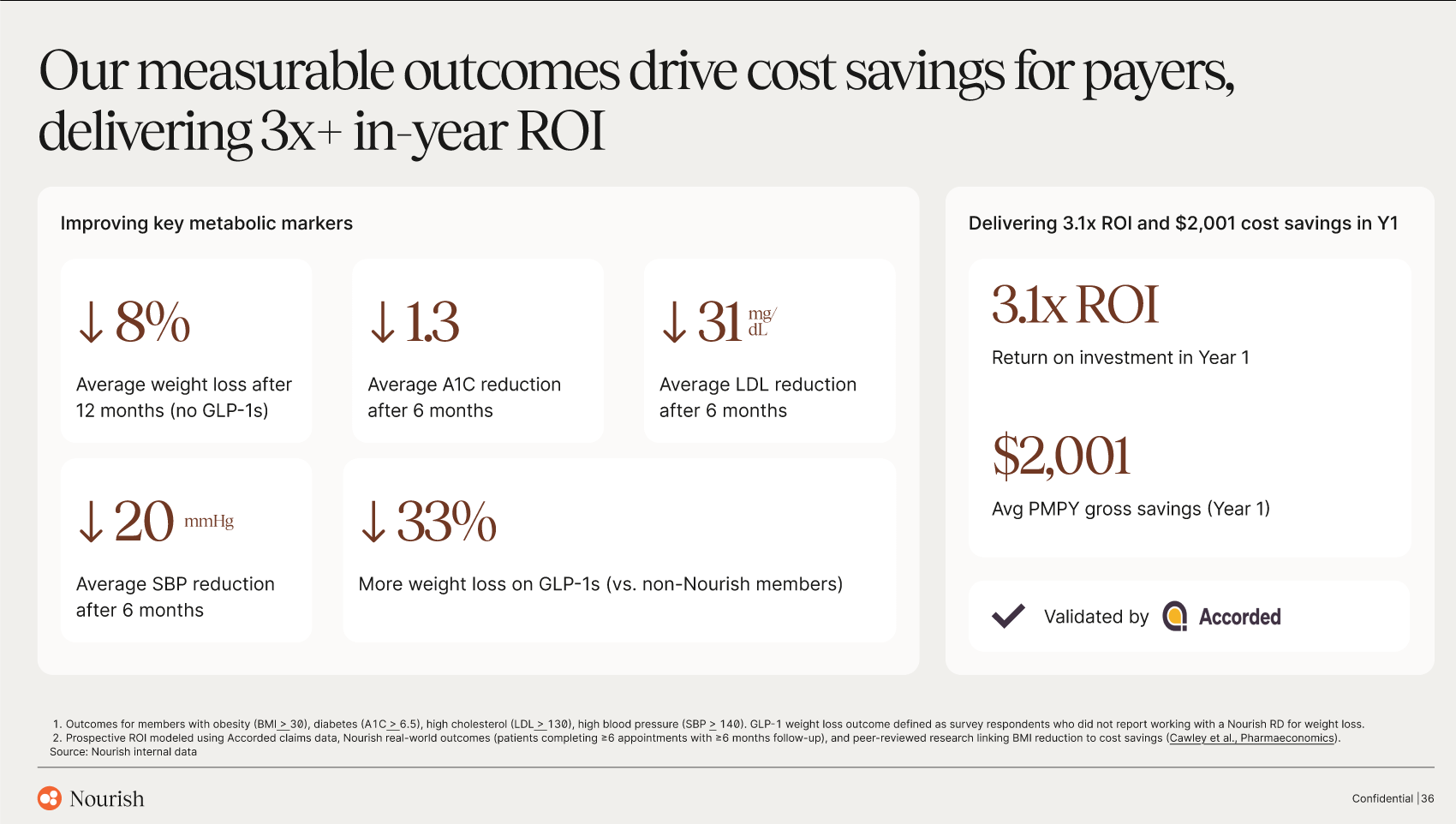
Nourish addresses this with an AI-native metabolic clinic, built to drive behavior change and measurable outcomes. The company drives real outcomes: 8% weight loss, 1.3 point A1C reduction, 31 point LDL cholesterol reduction, and 23 point systolic blood pressure reduction, resulting in over $2,000 per patient in annual cost savings for health plans.
One of my long-held views is that ideas are largely commodities (with rare exceptions), and that winning hinges almost entirely on execution. Execution, meanwhile, mostly comes down to velocity. The Nourish team has some of the highest velocity I’ve ever seen.
The VC cliche is that velocity, definitionally, is a function of speed and direction. You need to move fast, sure, but you also need to move in the right direction. Nourish has paired shipping speed with some key early insights that pointed them in the right direction.
Let’s break down three insights, one per side of the triangle:
1) Patients: Nourish built for consumers, but quickly diversified its channel mix away from DTC.
Starting in consumer forces healthcare companies to build a legitimately great product. Consumers are spoiled: we can call a black car on our phones, swipe to buy a stock, or have food delivered to our doorstep in a few taps. This means that increasingly, consumers are demanding that healthcare be just as design-forward, intuitive, and delightful.
Nourish began as a consumer company, and will always have its DNA in consumer. But the team also saw potential headwinds. Being over-reliant on DTC can lead to eroding CACs over tiem. Led by Sam, the Nourish team intentionally diversified their channel mix away from DTC. A huge and growing portion of acquisition now comes through providers, with tens of thousands of providers from over 250 health systems referring hundreds of thousands of patients to Nourish’s care model.
That channel is led by a 100-person field sales team, which Nourish is actively hiring for.
2) Providers: Build a workforce that’s 100% W2.
The prevailing wisdom in healthcare startups was to employ providers as 1099 workers. 1099 workers don’t require the employer to pay payroll taxes, benefits, malpractice insurance, and so on.
Nourish bucked this trend by employing RDs as W2 workers. The team made this decision with the belief that W2 would (1) ensure high-quality care for patients, and (2) ensure an attractive place to work for providers. Both have proven out. Quality of care is high and providers have extremely low churn. W2 workforces that maintain high-quality outcomes are also beneficial for payer contracts, which brings us to…
3) Payers: Strike national contracts with payers that improve margins and drive better patient costs / outcomes.
Nourish used its early traction to prove out ROI and sign payer contracts. The company has over 60 contracts covering 200M Americans.
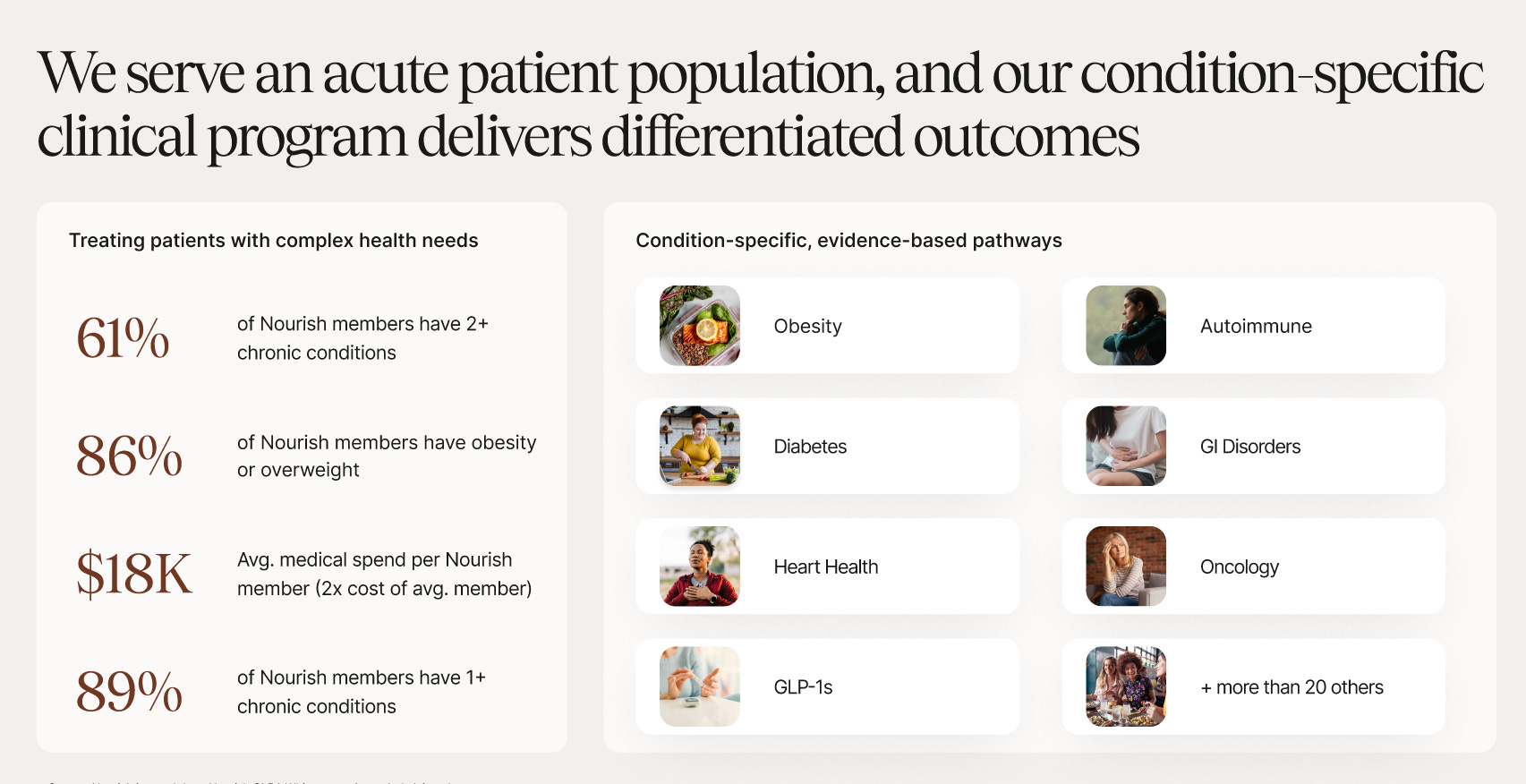
Importantly, Nourish’s patient population is a population that payers care deeply about: 61% of Nourish patients have 2+ chronic conditions, 81% are obese or overweight, and patients cost $18K per year in medical spend (2x the national average). Payers are working hard to help these people live healthier and happier lives.
The company has validated its ROI with third parties; you can see here that payers see 3x in ROI and $2,001 per member per year savings. Put more simply, Nourish’s payer and health system partners are happy to reimburse care because it saves them money down the road.
These three examples are each strategic decisions that set the team on the right course. They built a product that delivers real value to each side of the three-sided marketplace, and then sprinted to scale: more patients, more providers, better coverage. This is what enabled Nourish to become the leader in telenutrition, and laid the foundation for the care model expansion that’s defining their next act.
Roadmap (Where Nourish Goes From Here)
Many consumer healthcare companies have remained heavy on cash pay, forgoing the complicated and frustrating world of payers. In many cases, this has led to success. But it has also capped how large these companies can grow.
Nourish has gone through insurance from day one, which has unlocked a larger TAM and paved the way for something more ambitious than telenutrition. The roadmap from here is to expand from a dietitian-first product into a full-stack metabolic clinic, and eventually, into something resembling a new kind of healthcare system entirely.
Cardiometabolic dysfunction is the root cause of most chronic disease in America. There are the obvious culprits, like diabetes and heart disease, but also conditions you wouldn’t immediately associate with metabolism: autoimmune disorders, certain cancers, Alzheimer’s, anxiety, depression, even brain fog and fatigue. These are all different manifestations of the same underlying problem, and that problem exists downstream from lifestyle: nutrition, sleep, stress, and movement. If you fix the inputs, you fix a remarkable amount of what sickens Americans.
Our current healthcare system isn’t built to fix inputs. It’s reactive, built to diagnose, prescribe, and repeat. That made sense in 1900, when pneumonia, tuberculosis, and gastrointestinal infections caused a third of all deaths in America and the average newborn was expected to live to just 47. Reactive medicine was the right tool for that time, but it makes less sense in 2026, when most of what’s killing us is preventable, reversible, and rooted in how we live.
To tackle what’s on Nourish’s roadmap:
1) An integrated care team (vs. a point solution)
The team has been shipping rapidly on new products. Three example launches from Q4: Nourish Labs, Nourish Medical, and Nourish AI. Nourish Labs expanded into lab work, with over 100,000 labs completed after a Q4 launch. Nourish Medical brought in physician consults for labs, prescriptions, and complex conditions, integrated into Nourish care pathways. And Nourish AI is self-explanatory, but helps patients access 24/7 personalized guidance in the app.
These launches are laying the groundwork for an ambitious vision of integrated care.
Most digital health companies are point solutions: one provider type, one condition. This is essentially the digital version of the siloed system we already have, with all of its limitations. Nourish’s view is that the real unlock comes from integrating across the pillars of lifestyle medicine: integrated, multi-disciplinary care team; medications (eg GLP-1s, statins); data (via labs, wearables, devices); and AI.
This is also the thesis behind Nourish Medical, the physician layer launched in Q4. A wider surface area means better outcomes, more data, internal referrals, and stickier retention. It also means the company can responsibly incorporate medications (GLP-1s and other metabolic drugs) into a care model where the goal is to eventually taper patients off medications when possible. Aidan, Sam, and Stephanie would tell you that medications aren’t the enemy; the enemy is the wrong incentive structure around medications, and not pairing medications with lifestyle change.
There’s also a workforce angle to integrated care. Our current system burns out providers as much as it fails patients. Private practice has been hollowed out; most clinicians now spend more time on documentation than on care. The opportunity now is to build the system providers wish they worked in.
2) An AI-native product layer that consolidates patient health data
Healthcare data today lives across labs, devices, records, apps, and provider portals. None of it talks to each other, and the patient certainly doesn’t own it.
Nourish is building toward the opposite: a single, AI-powered front door where the patient owns their data and the system gets smarter the more they use it. Ingesting labs, wearables, meals, symptoms, habits, EHR data means building a real-time, longitudinal view of the patient. You can then pair that with an AI that acts as a 24/7 coach between visits, and as a copilot for providers during visits.
This is the “AI doctor for everyone” concept mentioned earlier, but with the addition of a real care team behind it. Human-in-the-loop is the right framing: AI handles what scales (admin work, routine questions, pattern recognition across data) and providers handle the less scalable human side (trust, nuance, judgment, hard conversations). The flywheel here compounds. More patients → more data → smarter AI → better outcomes → lower CAC → more patients.
3) A move toward value-based care
Today’s healthcare system pays for procedures, not outcomes. We’re volume-based vs. value-based. Incentives are upside down.
The fix is value-based care: getting paid for helping people live longer and feel better, rather than for treating them when they’re sick. To do that, you need scale and you need outcomes data. As Nourish widens its surface area across conditions, providers, and the pillars of lifestyle medicine, it lays the groundwork to eventually take on risk and to monetize differentiated outcomes the company drives.
Final Thoughts: Atomic Level of Impact
In the midst of all the metrics and business jargon we use in startups, it’s easy to forget the whole point of scaling: making sure more people get a great product or service. Nourish is serving hundreds of thousands of patients (3x year-over-year growth). While the overall number is impressive, that’s 100,000 unique human beings. It’s important to keep a pulse on the atomic level of impact that Priscilla Chan talked about.
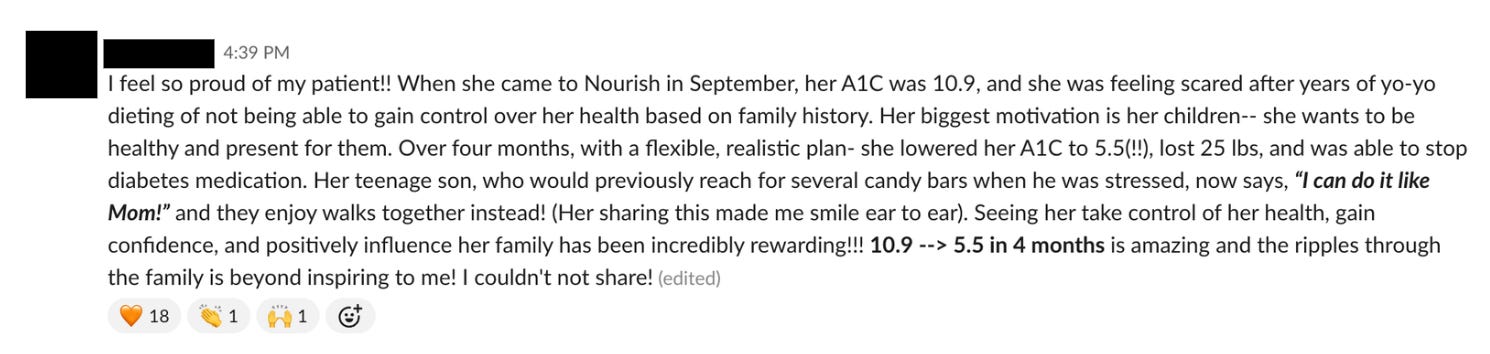
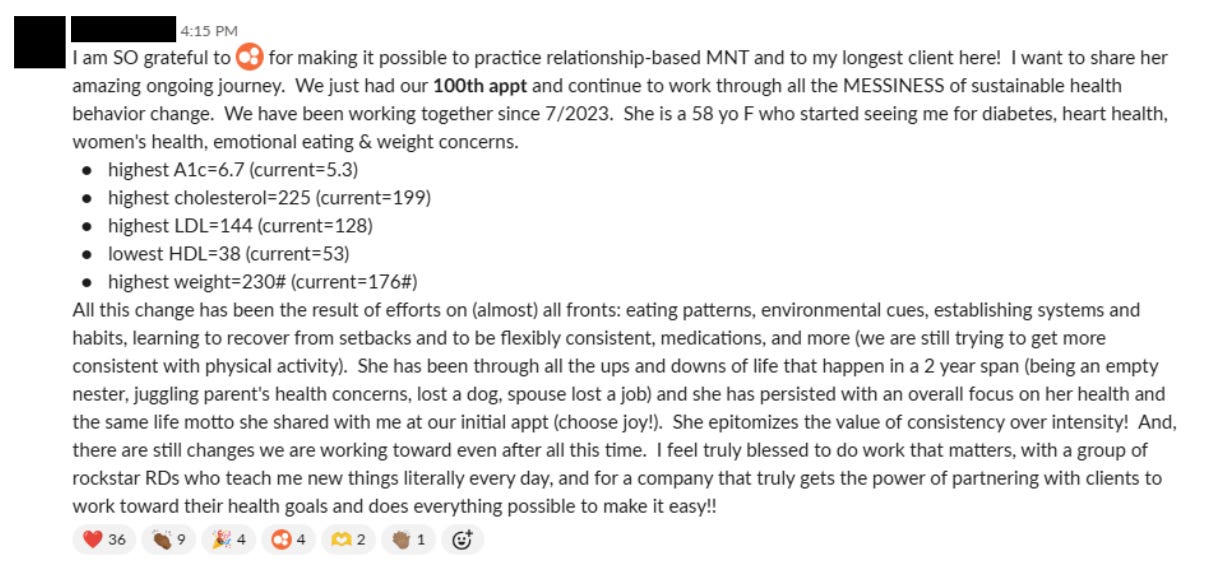
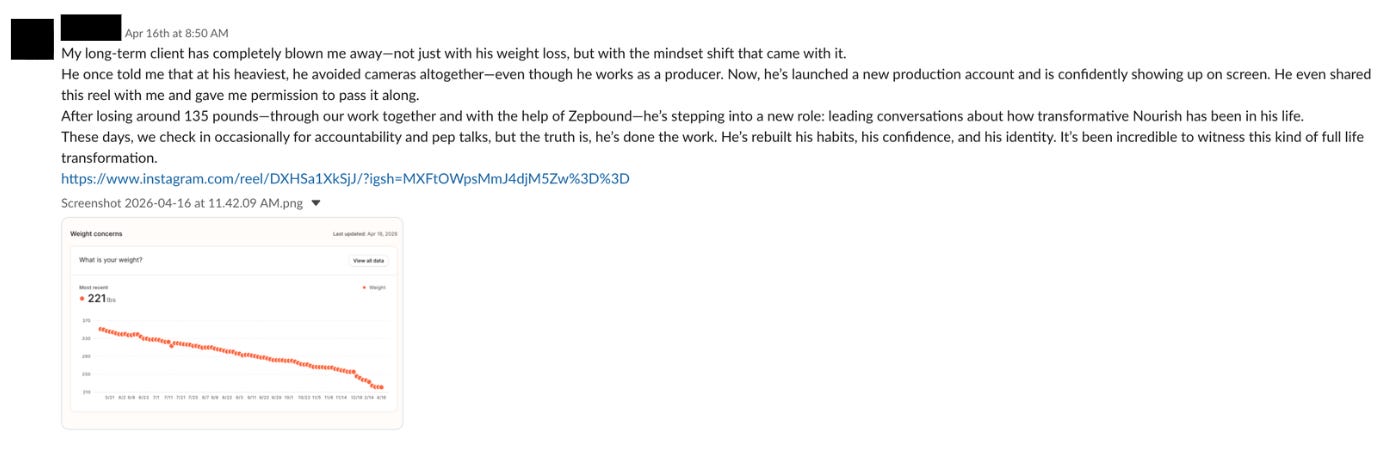
In that vein, let’s end with a few messages from Nourish team members sharing patient stories.
Thanks for reading! Subscribe here to receive Digital Native in your inbox each week:
